The Evolution of Healthcare Language
in America
How U.S. healthcare terminology changed — and what it says about the industry.
How U.S. healthcare terminology changed — and what it says about the industry.
American healthcare has a habit of reinventing itself through language.
Every decade seems to introduce a new vocabulary. Some terms disappear almost entirely. Others become so dominant that they start shaping how hospitals operate, how insurers make decisions, and even how patients are perceived.
What is interesting is that these terminology shifts are rarely accidental. They usually reflect something much bigger happening underneath: a financial transition, a political push, a technological breakthrough, or an operational crisis the industry is trying to solve.
If you look closely enough, the history of modern U.S. healthcare can almost be told through its changing buzzwords.
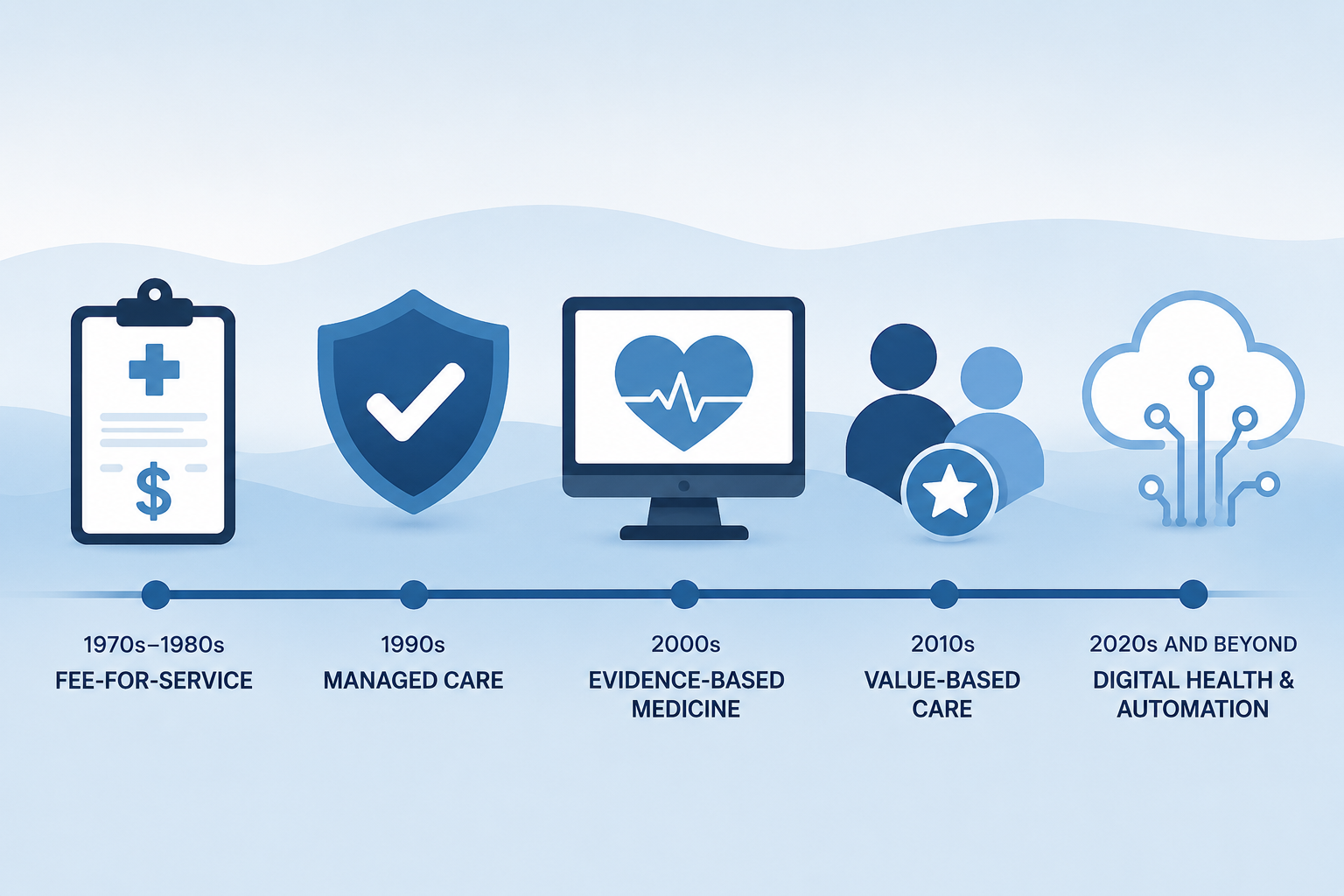
In the 1970s and early 1980s, one phrase dominated nearly everything: fee-for-service.
Healthcare was built around volume. More procedures meant more reimbursement. The system rewarded activity, expansion, and utilization. Hospitals grew rapidly, specialists multiplied, and healthcare spending exploded alongside them.
The language of that era reflected the mindset. Conversations centered around reimbursement, billing volume, utilization, claims, and procedures.
Very little attention was given to coordination or efficiency. The system was not designed to ask whether care was connected. It was designed to process as much care as possible.
By the 1990s, costs had risen so aggressively that the industry entered a completely different phase. Suddenly the dominant phrase became managed care.
This was more than a terminology change. It represented a philosophical shift in American healthcare. Insurers began introducing tighter controls around treatment decisions, referrals, network access, and medical necessity.
New operational terms appeared everywhere: utilization management, prior authorization, gatekeepers, coverage determination, and provider networks.
Even the word “patient” started changing in some business discussions. Patients became “members,” “covered lives,” or “consumers.” Healthcare was increasingly being viewed not only as clinical care, but as a system requiring financial oversight and behavioral management.
This was also the period when prior authorization became deeply embedded into healthcare operations. What started as a cost-control mechanism slowly evolved into one of the defining administrative structures of American medicine.
In the 2000s, another major terminology wave arrived: evidence-based medicine.
The healthcare industry was becoming more digital, more measurable, and more standardized. Clinical decisions increasingly relied on protocols, studies, guidelines, and quality metrics. Hospitals and payers wanted structured documentation and comparable outcomes.
Data became central to operational strategy.
This was the era when healthcare organizations started realizing that terminology itself mattered technically. Standardized coding systems, structured records, and interoperable data models became foundational infrastructure instead of background administrative tools.
Quietly, this period laid the groundwork for modern interoperability.
Then came the 2010s and one of the biggest healthcare buzzwords of the modern era: value-based care.
The phrase sounded simple enough. Healthcare should reward outcomes instead of volume. In theory, providers would be incentivized to keep patients healthier rather than simply performing more billable services.
But the language surrounding healthcare changed dramatically again. Suddenly everyone was talking about population health, care coordination, risk adjustment, quality measures, shared savings, and patient outcomes.
The Affordable Care Act accelerated this shift, and CMS heavily promoted the terminology across federal programs. Entire healthcare conferences became dominated by the phrase “value-based care.”
At the same time, many clinicians and administrators started questioning what the phrase actually meant in practice. Value for whom? Patients? Providers? Employers? Payers? Investors?
The terminology sounded patient-focused, but operationally it often translated into new reporting requirements, quality scoring systems, and reimbursement models.
Around the same period, another subtle but important language shift began happening. Healthcare organizations started moving away from terms like “non-compliant patient,” which sounded punitive and transactional.
Instead, phrases like “patient-centered care,” “person-centered care,” and “whole-person care” became increasingly common.
This was partly cultural, partly operational. The industry slowly recognized that language shapes relationships. Calling someone “non-compliant” frames the patient as a problem. Calling care “person-centered” frames healthcare as collaborative.
The change also reflected a growing awareness that healthcare outcomes are influenced by much more than clinical treatment alone. Social determinants of health, behavioral health integration, patient engagement, and care navigation became mainstream concepts.
Today, healthcare is entering yet another terminology cycle, driven largely by digital infrastructure and artificial intelligence.
Now the dominant phrases sound very different from previous decades. Healthcare conversations increasingly revolve around interoperability, FHIR APIs, digital health, workflow automation, ambient AI, payer-provider connectivity, care orchestration, and real-time data exchange.
The industry is slowly shifting away from simply digitizing paperwork toward actually connecting systems together.
That distinction matters.
For years, healthcare often replaced paper with portals. Instead of faxing forms, staff uploaded PDFs into web interfaces. Instead of calling for status updates, teams logged into multiple payer systems. The workflows became digital, but not necessarily connected.
New CMS mandates like CMS-0057-F and CMS-0053-F are pushing healthcare toward something more structured: standardized APIs, electronic attachments, and interoperable workflows that can move data directly between systems.
Whether the industry fully succeeds is still unclear. But the terminology already tells us where healthcare wants to go next.
Looking back, each major terminology shift in healthcare reflects the industry reacting to problems created by the previous era.
Fee-for-service created uncontrolled cost growth, which led to managed care. Managed care created administrative friction, which fueled evidence-based standardization and value-based care initiatives. Fragmented digital systems created interoperability mandates and automation efforts.
Healthcare language evolves because healthcare priorities evolve.
And sometimes the fastest way to understand where the industry is heading is simply to pay attention to the new words everyone suddenly starts repeating.
Healthcare terminology has always reflected the industry’s biggest problems.
Today, the language is increasingly centered around interoperability, automation, and connectivity — because modern healthcare is no longer struggling just with digitization, but with getting fragmented systems to finally work together.
Get practical Insights on Prior Authorization — no spam, just useful updates.
Subscribe