A 20-foot distance between a medical assistant and a prior authorization specialist can turn a process that should take minutes into one that takes hours.
Most clinics try to speed up prior authorization by adding new systems, automation, or more staff training. Those things can help. But one of the simplest causes of delay is often overlooked:
How the team is physically and operationally organized.
This affects how quickly questions get answered, how often errors happen, how long prior authorizations take, and ultimately, how much revenue is delayed or lost.
Example: A Small Pain Management Clinic
Let’s take a typical small pain management clinic:
• 2 physicians: a pain specialist and a physiatrist
• 2 medical assistants
• 1 prior authorization specialist
• 1 billing / RCM specialist
• 1 front desk employee
The clinic handles procedures such as injections, imaging, and interventional pain treatments — many of which require prior authorization.
In this kind of workflow, prior authorization often becomes the bottleneck.
What an Inefficient Setup Looks Like
In many clinics, the physical space appears organized on the surface:
• Front desk near the entrance
• Medical assistants working around exam rooms
• Prior authorization specialist in a separate office or back room
• Billing in another area of the clinic
But in practice, this creates slow, asynchronous communication.
A medical assistant sends a request. The PA specialist reviews it and finds missing information. They message or call back. The MA is already with a patient. The physician has moved on to the next visit. The answer gets delayed.
Every communication loop can add 30 to 120 minutes of delay.
By the time the issue is resolved, the case has lost momentum and often gets pushed to later in the day — or even the next day.
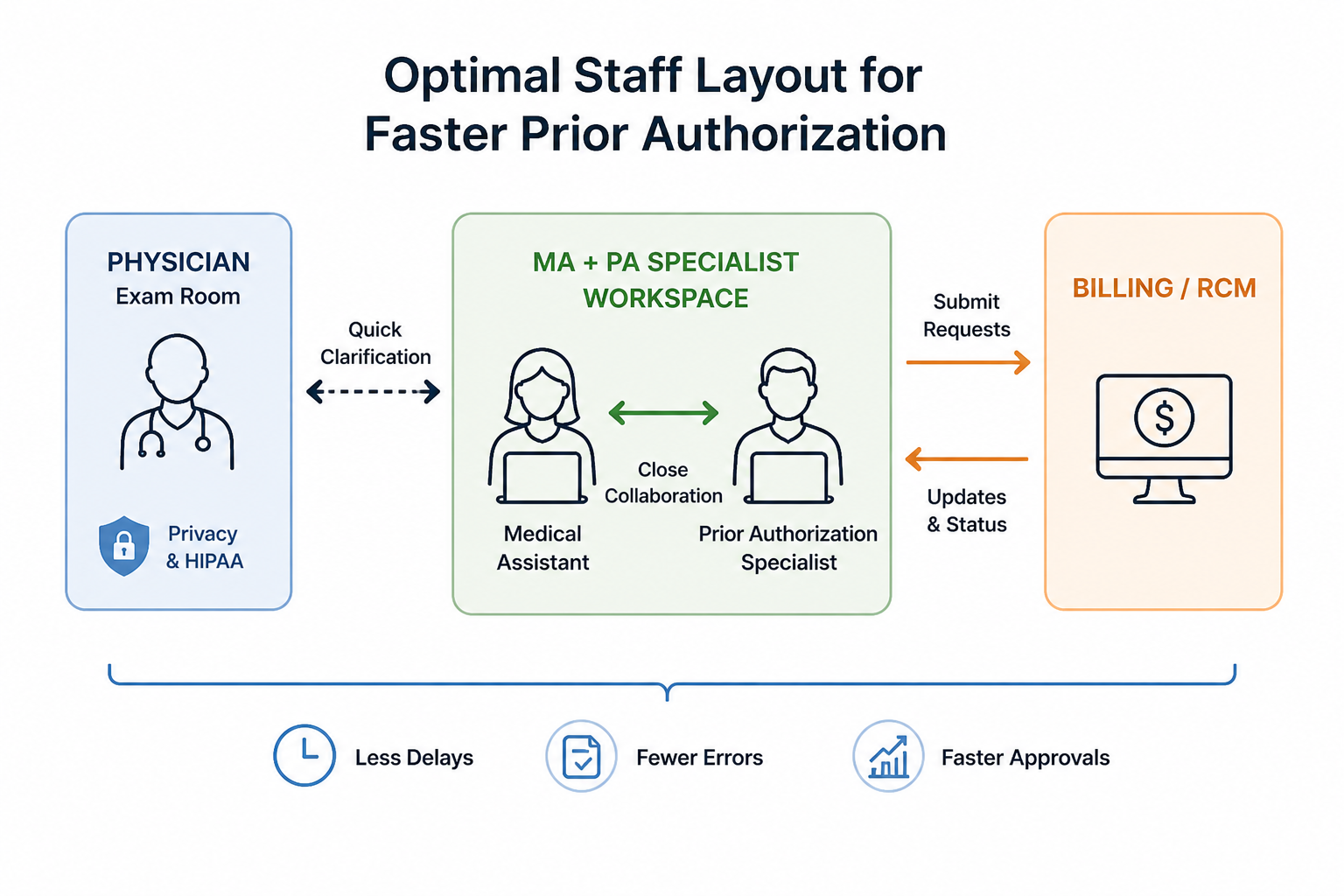
A Better Model: Fast Access Without Compromising Privacy
This does not mean the physician and prior authorization specialist should sit in the same room during a patient visit.
Patient exams require privacy, confidentiality, and proper HIPAA safeguards. That part is non-negotiable.
The key point is different:
The team should be able to reach the physician quickly outside the moment of the actual exam.
In practice, this means the physician remains in the exam room, while the medical assistant and PA specialist work in a nearby zone. The MA can quickly ask a short clarification question between visits, after knocking, stepping into the work area, or using an agreed-upon workflow.
The goal is not to remove privacy. The goal is to remove unnecessary waiting.
What a Fast Workflow Looks Like
In an optimized setup, the workflow is much smoother:
1. The medical assistant documents the case.
2. The MA turns to the PA specialist and asks:
“Does this payer require proof of failed conservative treatment?”
3. The PA specialist checks immediately.
4. The MA gets a quick clarification from the physician between patient interactions.
5. The PA specialist submits the request.
The total cycle can drop from hours to 5–10 minutes for routine cases.
Before vs. After
| Task |
Inefficient Setup |
Optimized Setup |
|---|
| Clarify with physician |
~45 minutes |
30 seconds to a few minutes |
| Fix missing documentation |
2–4 hours |
2–3 minutes |
| Routine PA cycle |
4–6 hours |
10–15 minutes |
| Errors due to missing or unclear information |
Higher risk |
Lower risk |
What About Remote PA Specialists?
Remote prior authorization specialists are common, and they can be very useful.
The advantages are clear: lower cost, flexible staffing, and easier scaling.
But there are tradeoffs. Remote PA work can create slower communication, more back-and-forth, weaker clinical context, and a higher chance that small documentation issues are missed.
In other words, savings on staffing can turn into losses in speed and quality if the workflow is not designed carefully.
The Best Practical Model: Hybrid
For many clinics, the best model is hybrid:
1. One onsite PA specialist
This person handles real-time questions, complex cases, physician coordination, and urgent issues.
2. Remote PA specialists for volume
Remote specialists can process routine requests, handle standardized cases, and help clear the backlog.
This gives the clinic both speed and scalability.
The Non-Obvious Insight
Many clinics assume the solution is simple:
“We need more staff.”
But often the real issue is not how many people are on the team. It is how quickly they can communicate.
You can hire another PA specialist. But if the same delays, messages, and handoffs remain, the workflow may not improve.
Sometimes the fastest improvement comes from changing the structure before changing the headcount.
The Financial Impact
Let’s say a small clinic handles about 300 prior authorizations per month.
If poor communication creates just 5% more errors, that means about 15 additional rework cases per month.
If each rework costs roughly $25–$40, that becomes:
• $375–$600 per month
• $4,500–$7,200 per year
And that does not include delayed procedures, lost patients, or services that are never billed.
Small communication delays can become real financial losses.
Why This Matters for Automation
Even the best automation cannot compensate for a broken workflow.
If information moves slowly, decisions are delayed, and clinical context gets lost, technology will not solve the problem by itself.
But when the team is organized correctly, tools start working the way they are supposed to:
• information moves faster
• decisions happen sooner
• missing documentation is caught earlier
• prior authorization requests become easier to complete correctly
A Quick 15-Minute Self-Check
Walk through your clinic and ask:
• Can the MA quickly reach the physician when clarification is needed?
• Does the PA specialist get answers without long waits?
• Are cases delayed because people rely on messages instead of quick clarification?
• Do cases get stuck between clinical documentation and submission?
• Are stalled requests visible before they become a problem?
If two or more answers point to delays, the workflow may be leaking time and money.
Final Thought
The physics of prior authorization is simple:
Distance creates delay.
Reduce unnecessary distance, improve access to the right people, and you reduce time, errors, and avoidable rework — without automatically hiring more staff.
What Comes Next
Once your team is organized correctly, the right tools become much more effective.
Instead of searching through payer portals or guessing what documentation is required, teams need a faster way to see:
• whether prior authorization is required
• what documentation may be needed
• where a case is likely to fail before submission
That is exactly what PriorAuthSpace is building — a simpler way to reduce guesswork and speed up prior authorization workflows.
Stay updated
Get practical Insights on Prior Authorization — no spam, just useful updates.
Subscribe